
Legislative Actions and Updates
An overview of the latest policy changes and updates impacting digital health.
Government Shutdown + Medicare Telehealth Waiver Cliff
On October 1, 2025, absent legislative action, the continuing resolution (CR) providing funding for the federal government will expire. Included in this CR was an extension of telehealth reimbursement flexibilities for Medicare to the same date, such as waiving geographic site restrictions and expanding the providers eligible for telehealth reimbursement.
CTeL is actively monitoring developments on this upcoming cliff and will include a special report in each week’s Policy Scoop newsletter leading up to the date.
Leaders are laying out their positions on a path forward.
The White House wants to see a CR through January 31st. This would not be a ‘clean’ CR keeping all funding the same – the Administration sent a 21-page list of ‘anomalies’ that it wants adjusted through any CR.
Congressional Democrats want to see an extensionof ACA tax credits set to expire at the end of the year, and it’s becoming an increasingly hardline position for the party.
Appropriators want time to put together a full slate of all 12 bipartisan-negotiated appropriations bills with a shorter CR of 1-3 months.
House Speaker Mike Johnson is interested in a more fleshed-out appropriations process - “What we’re really advocating for is an actual, old-school conference, the way this is supposed to work between the House and Senate.”
These conversations do not directly address telehealth but serve as an indication of how long Congress might provide for an extension of existing flexibilities. CTeL’s conversations with lawmakers indicates that there is little desire to see them expire – telehealth is broadly supported by Congress. There have been numerous bills introduced this year to provide for longer extensions of flexibilities, such as the CONNECT for Health Act and the Telehealth Modernization Act of 2025. Whether telehealth flexibilities become collateral in broader government funding fights remains to be seen.
CTeL is here to support your organization. Our Contingency Planning Worksheet reviews key financial and communications considerations for your organization and is intended to help you prepare for any potential expiration. We cannot say with certainty whether these flexibilities will be extended, and if so, for how long. We encourage our members to stay up-to-date on these developments and to get involved in CTeL community efforts, such as working groups and chapter meetings.
Want to talk more about this or any other policy issues? Email Lydia at lydiah@ctel.org, or schedule a time to meet here.
Understanding the CY 2026 CMS Physician Fee Schedule Proposed Rule
The Centers for Medicare & Medicaid Services (CMS) has released the Calendar Year (CY) 2026 Physician Fee Schedule (PFS) proposed rule, outlining significant potential changes to how physicians and other healthcare professionals are reimbursed for services provided to Medicare beneficiaries. This annual rulemaking process is critical for the healthcare community, and this year's proposal contains key provisions that will directly impact the delivery and expansion of telehealth services across the nation.
CTeL is actively analyzing the proposed rule and is committed to ensuring the voice of the telehealth community is heard.

What is the Physician Fee Schedule?
The Physician Fee Schedule (PFS) is the comprehensive list of fees that Medicare uses to pay doctors and other clinicians for their services. Each year, CMS proposes and finalizes updates to the payment rates, policies, and covered services. These updates can influence everything from the financial viability of a practice to the adoption of innovative care delivery models like telehealth.
Key Highlights in the CY 2026 Proposed Rule for Telehealth
While a full analysis is ongoing, the CY 2026 proposed rule introduces several important topics for discussion that could shape the future of virtual care. Key areas of focus include:
Telehealth Services List: Proposed additions or removals of services eligible for reimbursement when delivered via telehealth.
Reimbursement Rates: Adjustments to payment rates for telehealth services, including policies related to geographic adjustments and payment parity.
Supervision Requirements: Potential modifications to the requirements for direct supervision, which could allow for greater use of virtual technologies to supervise junior clinicians.
Behavioral Health: Continued focus on expanding access to virtual mental and behavioral healthcare, a critical priority for patients and providers.
Remote Therapeutic Monitoring (RTM): Proposed refinements to the coding and payment policies for Remote Therapeutic Monitoring services.
Understanding the nuances of these proposed changes is essential for any organization involved in providing or supporting telehealth services. The policies finalized in this rule will set the stage for telehealth operations in 2026 and beyond.
Telehealth Policy 411: What You Need to Know
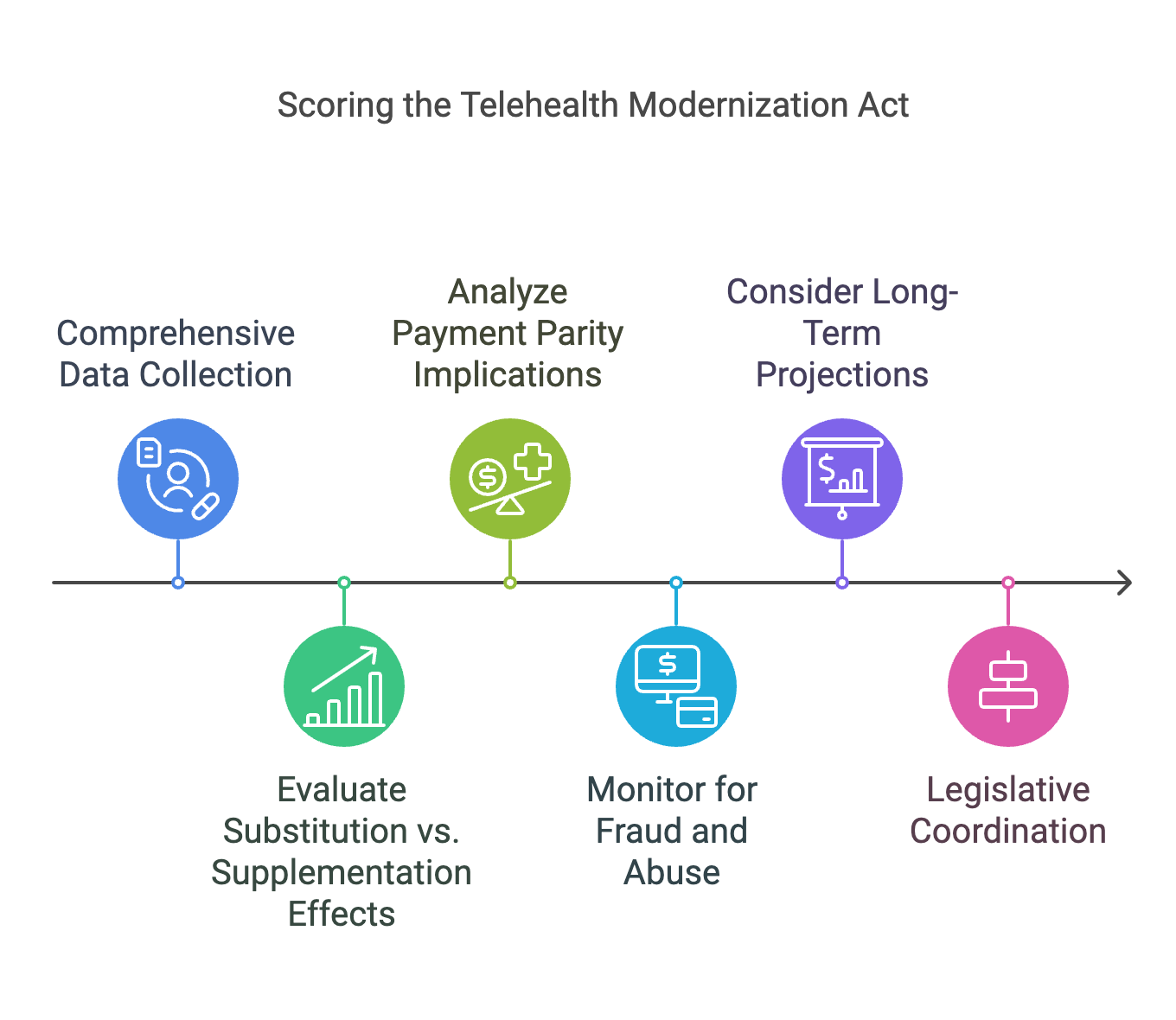
To secure legislation making telehealth access permanent, congress needs the right research and information for an accurate Congressional Budget Office (CBO) score. To accurately score the Telehealth Modernization Act (TMA) for its permanent implementation, Congress and the CBO should undertake the following steps:
Comprehensive Data Collection: Gather extensive data on telehealth utilization, costs, and outcomes. This includes analyzing spending patterns, service usage, and patient outcomes within Medicare, as well as reviewing studies on telehealth's impact on healthcare delivery and costs.
Evaluate Substitution vs. Supplementation Effects: Assess whether telehealth services replace in-person visits (substitution) or add to overall healthcare utilization (supplementation). Understanding this distinction is crucial, as increased utilization can lead to higher costs.
Analyze Payment Parity Implications: Examine the effects of reimbursing telehealth services at rates equivalent to in-person visits. Consideration should be given to whether this parity leads to increased utilization and spending, or if adjusted rates could better align with the cost structure of telehealth services.
Monitor for Fraud and Abuse: Implement measures to detect and prevent fraudulent activities within telehealth services. This includes establishing monitoring systems to identify outlier billing patterns and ensure compliance with healthcare regulations.
Consider Long-Term Projections: Incorporate long-term cost projections, potentially extending beyond the standard 10-year budget window, to fully capture the financial implications of making telehealth provisions permanent. This approach can provide a more accurate assessment of future costs and savings.
Legislative Coordination: Ensure that legislative proposals include detailed provisions addressing the above factors. Clear legislative language can facilitate a more precise CBO scoring process by outlining the scope, limitations, and intended outcomes of the telehealth services to be covered.
By following these steps, Congress can work with the CBO to develop an accurate and comprehensive budgetary score for the Telehealth Modernization Act, facilitating informed decision-making regarding its permanent implementation.

Subscribe to the Telehealth Scoop!
Get the latest telehealth policy news you need to know, right to your inbox. Stay up-to-date on all the latest CTeL happenings, events, actions, and more!